|
The clinical anatomy of the
respiratory tract starts at the external nares or nose. The pig has a large horn plate, perforated
by the two nares. This rostal plane or
rostrum is used as a rooting and exploration organ and combined with the neck
muscles is extremely strong. It is
not unusual to have areas of bruising or erosion to the dorsal tip of the
rostal plane. The nose is secondarily
supported by a bone in the nose – the rostal bone. There are few or no hairs on the external surface of the nares.
|
|

|

|
|
Detail
of rostal plane with the external nares
|
Cross-section
of the nose at the level between premolar 1 and premolar 2.
|
|
Interior to the nares is the
nasal cavity which is largely filled by the nasal turbinates. The nasal cavity is divided into two
sections by a cartilage septum the nasal septum, which is normally straight. In each of the two nasal chambers there
are two outgrowths, on from the dorsal wall as a pundulous outgrowth – the
dorsal turbinate and on the lateral wall of the nasal chamber and complex
biscrolled structure the ventral turbinate.
If the nasal chamber is sectioned in a transverse plane between premolar
1 and premolar 2 the ventral turbinates effectively fill the entire nasal
chamber in the normal pig. The
position of the premolar 1 and premolar 2 is indicated by the lateral
commissure of the mouth.
The back of the upper
respiratory tract is the tonsils which act as a major lymph node sampling
both food and materials brought from the nasal chamber and the
trachea/bronchi. The surface of the
turbinates are covered in a mucocilary escalator which moves from the nares
to the tonsils and oesophagus where the mucus is swallowed and the material
killed by the acidic environment.
|
|
The middle respiratory tract is
defined by the larynx which lies at the root of the tongue. The pig has a large epiglottis which during
eating completely protects the entrance of the trachea allowing the pig to
eat and breath at the same time.
|
|

|
|
|
Root of the tongue and larynx
|
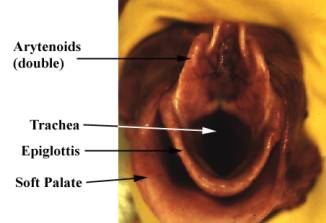
The entrance to the larynx (hand held)
|
|
Ventral to the large epiglottis
is a paraepiglottis fold, which can be troublesome when intubating a
pig. Intubation is difficult because
the larynx can be difficult to visualize as the pig does not have a wide
gape. During intubation the tube may
miss the larynx and enter the paraepiglottis fold, confusing the clinician
into thinking intubation has been successful. Note that in the pig the arytenoids are double.
|
|

|
|
The general layout of the chest with the ventral
surface removed.
|
|

|
At postmortem the respiratory tract
should be removed by making an incision along the medial border of the
mandible cutting through the hyoid apparatus and releasing the tongue. Pull
the tongue caudally and dissect the larynx and through the chest inlet. The lungs should easily strip away from
the pleura.
The incision
should be continued through the diaphragm ultimately to the rectum.
The photograph left
demonstrates the “pluck” without the liver and intestines attached.
|
|
The trachea starts below the
larynx. The trachea is supported by
incomplete cartilaginous rings. This
assists the clinician as once the larynx is incised the incision can easily
be continued right to the bottom of the right and left major bronchi to the
bottom of the lung.
|
|

|

|
|
Detail
of tracheal rings
|
Detail
of right tracheal bronchus
|
|
The trachea has three major
bronchi, a small right tracheal bronchus which feeds the right apical lobe and
the two major bronchi each which feed the rest of the lung. Clinically the right apical lobe is
important as this part of the lung is nearest the tonsils and is most
susceptible to descending pathogens – for example it is often the most
consolidated area in cases of enzootic pneumonia.
|
|

|
|
Detail
of end of bronchi cut surface at the caudal position in the lung.
|
|

|
The turbinates, trachea and bronchi are lined by a cells
covered in cilia. On the surface of the
cilia is a mucus layer. This layer,
captures in falling particles between 3 and 1.6 mm in size. These particles are then moved by the
cilia caudally from the nose to the throat or cranially from the lower
bronchi to the throat. The
mucociliary escalator is a major component of the defense of the respiratory
tract.
|
|

|
|
Lungs
dorsal view
|
|

|
|
Lung
ventral view
|
|
The lung can be easily divided
into seven distinct lobes – right and left apical, cardiac and diaphragmatic together
with the accessory lobe (visible on the dorsal view). During a clinical examination each of
these lobes should be examined in detail.
The surface of each lobe should be examined for pleurisy. Note the right apical lobe, as described
previously. The lung may require to
be further dissected to reduce its bulk to allow adequate palpation. The bronchial lymph nodes (of which there
are several) should be noted in the mediastinum on the ventral surface after
manual partition of each lung.
|
|
Once the lung is examined in detail, examine the
heart. If there is no gross evidence
of any blood vessel abnormalities, such as a patent ductus, remove the heart
from the respiratory pluck.
Peal away the pericardial sac and examined for
pericarditis. Open the heart using
four incisions:
- Incise into the right
auricle and continue the incision into the right venticle cutting
through the right AV valve. Keep
the incision close to the interventiculum septum.
- Incise into the left
auricle and continue the incision into the left venticle cutting through
the right AV valve. Keep the
incision close to the interventiculum septum.
- Using the point of
the scissors, find and cut into the aorta from the left ventricle
- Turn the heart over, find
and cut into the pulmonary artery from the right ventricle.
The heart can now be examined in detail noting the
pericardial wall, the right and left AV valves, noting any abnormality of the
interventricular septum and finally the pulmonary and aortic valves.
|
|

|

|
|
Parietal surface of the heart dorsal view
|
Parietal surface of the heart ventral view
|
|

|
|
Heart opened, right side.
|
|

|
|
Heart opened, left side
|
|
The pleura covers both the surface of the lung and the inner
wall of the chest. It should be
examined in detail for signs of pleurisy.
|
|

|
|
|
|
|
|